
 Native Health Issues
Native Health Issues
There are several articles on this page.
Look for the following pages: Census Facts (Health Disparities – at the bottom of the Census Information); Smallpox; PCB; Teen Suicide:Diabetes; Health Bill & related issues; Tradition & Science; PTSP in Vetrans
Related articles include: Women’s Health Issues in Native Women section; Socio-Political Issues
Health, Crime, and Doing Time: Potential Impacts of the Safe Streets and Communities Act on the Health and Well-Being of Aboriginal People in B.C., a new report by provincial officer of health Dr. Perry Kendall, says the Tory administration’s approach will exacerbate what is already a crisis.
In B.C., aboriginal women account for 26.4 per cent of the women in custody, according to Kendall. Native girls account for 56 per cent of juvenile females in custody. Native youth make up only about eight per cent of the provincial juvenile cohort, he added, but 142 of the 325 juveniles in custody are aboriginal. Read more: http://www.vancouversun.com/life/Soaring+aboriginal+prison+population +national+disgrace/8168948/story.html#ixzz2RyXL45du ***********************************************************************************************************************
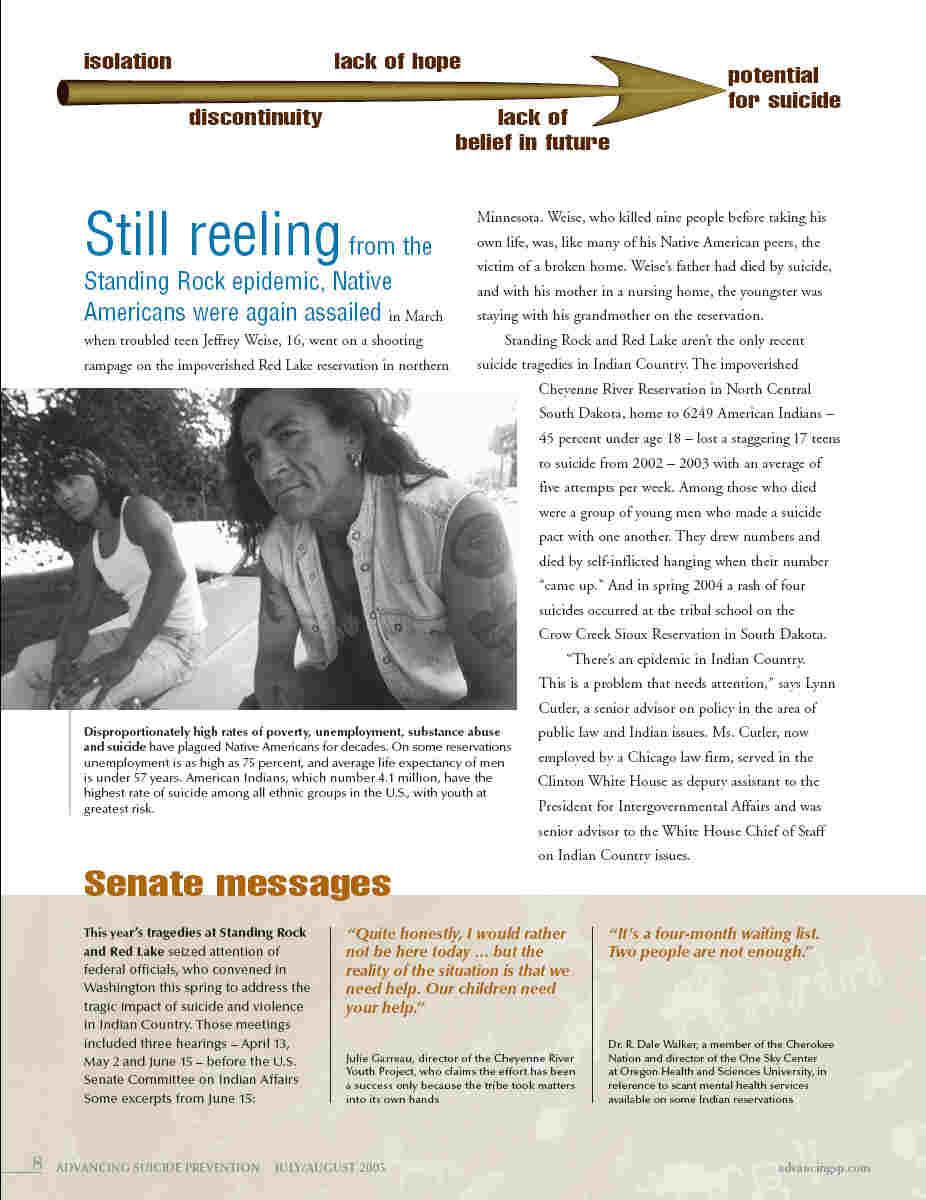
 Native Teen Suicide Read the full article at: Advancing Suicide Prevention http://www.advancingsp advancingsp.com/ASP_July_August_2005.pdf#page=9 11/3/05
Native Teen Suicide Read the full article at: Advancing Suicide Prevention http://www.advancingsp advancingsp.com/ASP_July_August_2005.pdf#page=9 11/3/05

![]() Access to Quality Healthcare Not Improving for Native Americans and Other Groups By Michelle Tirado · 03/04/2011 · American Indian Report – Falmouth Institute
Access to Quality Healthcare Not Improving for Native Americans and Other Groups By Michelle Tirado · 03/04/2011 · American Indian Report – Falmouth Institute
While the quality of healthcare in the United States is improving, albeit at a snail’s pace, disparities based on race/ethnicity, socioeconomic status and other factors have hardly budged, according to the recently released 2010 National Healthcare Disparities Report.
The report, published every year since 2003 by the U.S. Department of Health and Human Services’ Agency for Healthcare Research and Quality, looks at the status of healthcare quality and disparities in the nation, how they have changed over time and where the needs are for improvement.
It uses a group of more than 200 core measures that are categorized in several areas of quality: effectiveness, patient safety, timeliness, patient-centeredness, care coordination, efficiency, health system infrastructure and access.
Across all 179 measures of healthcare quality, nearly two-thirds showed improvement, the 2010 report said. The median rate of change was 2.3 percent per year.
The story was different for access to care, which showed no improvement in about 60 percent of 22 measures. In fact, the other roughly 40 percent were heading in the other direction, the report stated. The median rate of change: -0.6 percent per year.
Few disparities faced by race/ethnic groups are getting smaller. Less than 20 percent of those gaps faced by American Indians/Alaska Natives, as well as Blacks, Hispanics and the poor people, showed signs of narrowing. The Asian/White gap narrowed for about 30 percent of the core measures.
The report found that Blacks and AI/AN people received worse care than Whites for about 40 percent of the core measure, compared to 20 percent for Asians, 60 percent for Hispanics and 80 percent for low-income people.
AI/AN and Asians had worse access to care than Whites for one of five measures, compared to one-third of the measures for Blacks, five out of six measures for Hispanics and all six measures for poor people.
The hefty report is available online in PDF format. Copy & paste this link in your browser http://www.ahrq.gov/qual/nhdr10/nhdr10
The infant mortality rate is 150 percent greater for Indians than for Caucasians.
Indians are 2.6 times more likely to be diagnosed with diabetes.
Life expectancy for Indians is nearly 6 years less than the rest of the U.S. population.
Suicide for Indians is 2 1/2 times higher than the national average.
Indians have fewer mental health professionals available to treat them than does the rest of the U.S. population.
U.S. health-care expenditures for Indian men, women, and children are less than half of what the government spends on the health of federal prisoners.
American Indian/Alaska Native people (AI/ANs) had the 2nd highest diabetes death rate in 2003, the highest death rate from Chronic Liver Disease and Cirrhosis, were 1.5 times more likely to die from unintentional injuries.
American Indian and Alaskan Natives teens and young men have the highest suicide rate in the 15 to 24 age group and adult men the second highest rate of suicide after whites (CDC 2004).
The top five causes of death are heart disease, cancer, unintentional injuries, diabetes and stroke. Web Master Note: Things are not better!
Urban Realities
About 70 percent of Native Americans live in urban areas, according to the U.S. Census. Many Native people, although sometimes thousands of miles away from their traditional homeland, still speak their languages or maintain ties with their reservation or Indian communities, but often with some struggle.
American Indians in cities face unique challenges to their health By Garnce Burke Fresno, California (AP) 3-08 News From Indian Country 4/08
Urban American Indians face a health problem unseen by other races, researchers said during March: As they become wealthier, their rates of binge drinking and tobacco use stay the same or even rise.
The nonprofit Urban Indian Health Institute also said diabetes and obesity rates were about the same for urban Indians, whether they were rich or poor. Among other races, people with higher incomes tend to have fewer of those health problems than poorer people.
“When Indian folks drink, it appears to have nothing to do with how much money they have, and that’s not true for any other racial group,” said Maile Taualii, the institute’s scientific director. “There seems to be a sense of hopelessness, a sense that diabetes, alcoholism and other health problems are inevitable in the community, and it doesn’t have to be that way.”
The Seattle-based institute, which gets federal money to track disease trends among native people, analyzed data from a random digit-dial telephone survey conducted between 2001 and 2005 by the U.S. Centers for Disease Control and Prevention in 34 cities from New York to Helena, Mont.
More than half of the roughly 2.5 million American Indians in the United States live in cities, according to the 2000 Census. Yet rarely have medical studies focused on the population’s health as compared to other city dwellers, or to illness rates among Indian people living on tribal lands.
The report offers a detailed analysis of responses from the 3,224 American Indian and Alaska Natives and 178,983 non-Indians surveyed.
Overall, fewer Indian respondents reported drinking than people of other races. But among those who did drink, more American Indians reported an episode of binge drinking – or consuming five or more drinks in one go – at least once in the previous month.
Of higher-income respondents – defined as those earning more than $38,700 for a family of four – 46 percent of American Indians reported one episode of binge drinking in the previous month, compared with 25.3 percent for people of other ethnic backgrounds.
Taualii said the results of the study – and data showing that native people in some cities reported having more difficulty getting health care than urbanites of other backgrounds – show special attention must be paid to the health disparities for urban Indians.
Federal law requires taxpayer-funded tribal clinics, but the Bush administration has been pushing for those services to be cut off in urban areas. For the third year in a row, Bush’s 2009 budget proposal calls for the Urban Indian Health Programs’ funding to be cut.
Unlike American Indians who live in rural areas or reservations, “urban Indians have access to publicly and privately financed health care services like other Americans,” said Christin Baker, a spokeswoman for the White House’s Office of Management and Budget.
Newman Washington, who runs drug and alcohol programs at a government-funded Indian clinic in Wichita, Kan., said tight finances already make it difficult to meet the needs of patients from nearby tribes, including the Kickapoo, Potawatomi, Iowa, and Sac and Fox.
Clients trying to detox from alcohol often have to wait two months to be admitted to a hospital bed, or travel 75 miles to Ponca City, Okla., to be seen in an inpatient facility, Washington said.
“People go away and get an education, but then they come back home and have a really hard time changing their behavior,” said Washington, a member of the Eastern Shoshone tribe of Wyoming. “Whenever you start looking at the core, there’s some shame and guilt that people are carrying around from past generations.”
Officials at the U.S. Department of Health and Human Services, which oversees the urban clinics, did not return messages seeking comment on the study. Staff members for the Senate Indian Affairs Committee were examining the report, a spokesman for its leader, Sen. Byron Dorgan, D-N.D., said Wednesday.
Rep. Nick Rahall, D-W.V., said in a statement that the report “makes it clear that far too many disparities exist between those Native Americans living on A bill approved by the Senate last week would boost programs at the federally funded Indian Health Service, prompt new construction and modernization of health clinics on reservations and attempt to recruit more Indians into health professions.
Significant Health Care Needs of American Indians and Alaska Natives Living in Urban Areas Go Unmet
November 01, 2007 – Washington, D.C.
Urban Indian Health Commission reveals that urban Indians face a high incidence of heart disease, diabetes and depression, yet have minimal access to quality health care.
Millions of American Indians and Alaska Natives living in or near cities throughout the United States are seemingly invisible to health care providers and federal and state policy-makers and yet face significant heath care disparities, according to a new report, Invisible Tribes: Urban Indians and Their Health in a Changing World. The report will be released today by the Urban Indian Health Commission (UIHC), a select group of leaders convened by the Robert Wood Johnson Foundation and the Seattle Indian Health Board’s Urban Indian Health Institute to examine health care issues facing urban American Indians and Alaska Natives.
Nearly 67 percent of the nation’s 4.1 million self-identified American Indians and Alaska Natives, or about 2.8 million people, call U.S. cities home. However, there is no uniform policy regarding urban Indian health, and current federal executive policy actually aims to eliminate funding for urban Indian health within the Indian Health Service.
“The collective health of this growing population continues to suffer, and disproportionately, compared to other Americans,” said Ralph Forquera, M.P.H., director of the Urban Indian Health Institute. “The Commission’s report illustrates the need for health care providers; policy-makers; and local, state and national private and public sector leaders to work together to provide better care to this seemingly invisible population.”
The report reviews the prevalence of three diseases—depression, diabetes and cardiovascular disease—in the American Indian and Alaska Native population. Top-line findings from each disease include:
Up to 30 percent of all American Indian and Alaska Native adults suffer from depression, and there is strong reason to believe the proportion is even greater among those living in cities.
Compared to the general U.S. population, American Indians and Alaska Natives have a higher prevalence of diabetes, a greater mortality rate from diabetes and an earlier age of diabetes onset.
Cardiovascular disease is the leading cause of death among American Indians and Alaska Natives and kills more American Indians and Alaska Natives age 45 and older than cancer, diabetes and unintentional injuries—combined.
According to the report, it is common for an urban Indian to suffer from more than one of the aforementioned diseases, which ultimately interact with, amplify and perpetuate one another. Many of the underlying causes, markers and barriers to treatment of these diseases are shared, at above-average rates, by other diseases and afflictions suffered by American Indians and Alaska Natives.
A big challenge for urban Indians is accessing high-quality, appropriate health care. The vast majority of American Indians and Alaska Natives living in cities are ineligible for or are unable to use health services offered through the Indian Health Service or tribes. And even when urban Indians do manage to access health care, they must overcome additional barriers to receiving appropriate care. Cultural misunderstandings, a lack of respect and communication obstacles often interfere with—and inhibit—the delivery of high-quality health care to urban American Indians and Alaska Natives.
“We can’t ignore this population in our efforts to improve the quality of American health care,” said Michael W. Painter, J.D., M.D., senior program officer at the Robert Wood Johnson Foundation. “The nation cannot truly improve health care quality without also reducing disparities. Although we continue to make some in-roads in reducing racial and ethnic disparities in health care, these efforts have largely overlooked American Indians and Alaska Natives living in or near cities. We must make sure that the work to reduce disparities and improve the quality of care explicitly includes our nation’s first people, no matter where they might currently live. If we don’t, future generations will and certainly should judge us harshly.”
The UIHC report recommends informed dialogue and targeted action. The public and private sectors must recognize and assist urban Indians in order to improve their access to appropriate care and health services, work to enhance data collection and research pertaining to American Indians and Alaska Natives living in cities, support funding initiatives, and identify and institute best practices in urban Indian health care. Most importantly, Americans must understand that the quality of health care for all will not improve without addressing—and reducing—disparities.
“Decades ago, tribes exchanged their land and its vast resources for federal promises of better life and better health,” Forquera said. “The government has not delivered on its promise. We, as a nation, have a duty to right these wrongs, and illuminate this invisible population.”
The Urban Indian Health Commission is a select group of leaders convened by the Robert Wood Johnson Foundation and the Seattle Indian Health Board’s Urban Indian Health Institute to examine health care issues facing urban American Indians and Alaska Natives.
The Urban Indian Health Institute (UIHI) was established in July 2000 as a division within of the Seattle Indian Health Board, a community health center targeting urban American Indians and Alaska Natives. The UIHI provides centralized nationwide management of health surveillance, research and policy considerations regarding the health status deficiencies affecting urban American Indians and Alaska Natives.
The Robert Wood Johnson Foundation focuses on the pressing health and health care issues facing our country. As the nation’s largest philanthropy devoted exclusively to improving the health and health care of all Americans, the Foundation works with a diverse group of organizations and individuals to identify solutions and achieve comprehensive, meaningful and timely change. For more than 35 years, the Foundation has brought experience, commitment and a rigorous, balanced approach to the problems that affect the health and health care of those it serves. When it comes to helping Americans lead healthier lives and get the care they need, the Foundation expects to make a difference in our lifetime.
Contacts for Journalists Jared Harrison jared.harrison@gmmb.com Office: (202) 572-2866
Return to Top